"[..] our health and wellness is not simply a responsibility of the state but something we must work toward as individuals, families and communities, and as a nation."
Roy Romanow
Open source and communications enabled applications (CEAs) are emerging as a vital part of e-Health strategies across Canada. This article provides an overview of lessons learned from our investigation of collaborative telehealth systems delivery in Canadian healthcare. Specifically, the role of open source software (OSS) and CEAs with respect to pan-Canadian patient record management and telehealth service prototyping are discussed.
Challenges in Healthcare Delivery
Within the broader blanket of e-Health, which includes health record management, telemedicine has emerged as a unifying power in a largely fragmented system of healthcare delivery in Canada. However, many healthcare service-delivery companies are too small to support the research and development (R&D) requirements of the business on their own, and require partnerships in order to succeed. In combination with mature open source stacks, CEA-based healthcare applications provided by ecosystem partnerships and open collaboration hold promise for needed increases in service interoperability and scalability. Open source component stacks are finding their way into Canada's strategy for creating a cross-country Electronic Health Record (EHR), and for good reason. Some EHR success stories have been publicized in recent years, most notably, the Alberta Netcare system. However, many ambitious, large-scale information technology (IT) infrastructure overhaul projects undertaken by public organizations have been plagued by project cost and scheduling overruns. As a result, many industry experts are calling for a renewed focus on small-scale systems that:
-
demonstrate positive results early-on
-
start small, but can scale
-
make better use of OSS tools
Like many industrialized nations, the accelerated adoption of telemedicine in Canada is fueled by an aging workforce, demand for equitable and timely access to quality services, and a relative shortage of professional practitioners. This last factor is particularly noticeable in remote and rural communities in Canada. Lengthier wait times to access specialists in the healthcare system and increasing demand for treatment of chronic illness are by-products of these changing conditions.
Home-based telehealth provides the ability to connect scarce specialists with geographically-separated patients. By accommodating patients in their home environment, remote-monitoring systems eliminate a large portion of the travel time required for some home care. Supervising nurses are able to monitor more patients at once, while also increasing overall care by increasing the number of vital checkpoints.
Despite considerable demand for more efficient, customizable, and scalable healthcare solutions, many regional services struggle to find sustainable support models. The former Canadian Society of Telehealth highlights the lack of consistent reimbursement guidelines as an ongoing barrier to success for telehealth within most provincial jurisdictions. Most physicians participate in such services on a per-fee basis, outside of the standard reimbursement process. The agency further recommends that all provinces and territories explicitly reflect telehealth services within fee schedules for physicians. Some provinces, such as Nova Scotia, have managed to institute consistent funding, partly through the help of federal agencies such as Canada Health Infoway (CHI), for telehealth expansion and operations using fee-based reimbursement policies and are currently synchronizing their Picture Archiving and Communication System (PACS) and hospital IT infrastructure systems. On a national scale, however, EHR interoperability remains a challenge. CHI's Blueprint calls for EHR-ready IT and telehealth systems that provide:
-
point-of-service access to a shared EHR system, which is itself a collection of synchronized infostructures within provincial domains
-
applications that make use of shared EHR data, but cache operational patient data specific to local systems
Health Record Initiatives
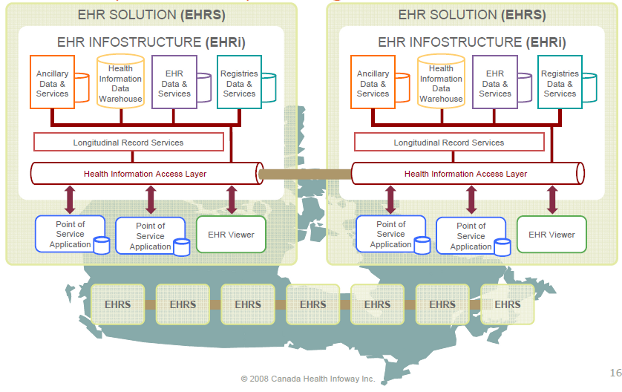
A major part of telehealth strategies, as well as most anything labeled e-Health, is the EHR. The need to search and share patient profile data is required by every telehealth service in Canada. Typically, these functions are managed through one or more IT systems that access data contained within a patient's EHR profile, depending on the level of regional or provincial coordination involved. In recent years, the idea of developing a pan-Canadian EHR strategy has taken center-stage in discussions about improving equitable access to medical services, a key tenet of Medicare. Canada's vision, largely driven by the federally-funded non-profit CHI, could be described as a system of unified fragments of existing or in-development regional records-management solutions, as shown in Figure 1.
Figure 1: CHI's Infostructure Vision
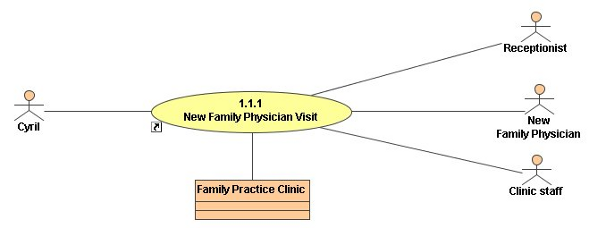
A tie-in for the standards-first message promoted by the CHI is the EHRS Blueprint. The Blueprint depicts user storyboards which are diagrams that map a patient's interaction with the medical community throughout the continuum of care across professional domains. Figure 2 provides a storyboard representing a patient's first visit within the chronic obstructive pulmonary disease treatment domain.
Figure 2: Storyboard Representing First Patient Visit
From an implementation perspective, the CHI does not stipulate a great deal of technical requirements for its paid service provider members. Instead, it provides access to licensed standards material such as HL7 and SNOMED CT. By providing guidelines and best-practice documentation, CHI hopes to build an interoperable patchwork of infostructures across the country that professionals can tap into. The push to use a messaging standard like HL7 is not a revolutionary concept, as most EHR solution providers support it, but it does encourage interface efficiency when designing integrated telehealth services.
The Infoway Reference Implementation Suite (IRIS) is arguably the most important initiative to emerge from CHI's game plan, from an entrepreneur's perspective. IRIS, released under an academic open source license, ratifies the HL7 protocol stack by leveraging a veritable who's who of open source components. Providing a layer of abstraction between application and data sources with IRIS might be the right ticket for many small entrepreneurs to contribute a compatible piece to an otherwise complex and distributed infrastructure. Learning from Alberta and Nova Scotia's experiences in expanding their regional IT systems to support a common EHR, CHI's approach to support both large and small players to drive the next-generation of user-centric, innovative telehealth solutions is forward-thinking. By not restricting providers to a single, all-encompassing format, they are opening the door to more efficient ways to manage and share patient data regionally and across Canada. A quick scan of open source EHR projects on Wikipedia reveals a list of at least 28 separate initiatives to create a standard record format for various healthcare domains. Even some early hierarchical database pioneering projects, such as the over-40-years-old MUMPS, are finding new life in today's collaborative environments.
Prototyping Telehealth Innovation with Open Source and CEA APIs
Beyond EHR, community-driven telehealth initiatives anchored on other open source components and CEAs may address some of the long-tail requirements and funding limitations felt by regional operators. In the context of telehealth, prototyping is manifested through process and protocol testing in clinical trials. Considering the legacy of top-down, large-scale projects in healthcare, such as videoconferencing infrastructure deployment, application prototyping is likely to increase in popularity as providers focus on customized solutions for segment markets at the end of the long tail and bottom-up scaling of solutions. Building telehealth services with open source software components invites the use of prototyping through low-cost experimentation of design. One such prototype telehealth application, is outlined in Figure 3. In this case, the simple application could be used to setup and schedule call-outs of patient-centric questionnaires that aim to reduce the likelihood of early hospital re-admission due to a patient's non-compliance with their medication. In the described prototype, a service provider could leverage the open source asterisk PBX and call-session management functions through open application programming interfaces (APIs) supported by third-party providers such as Coral CEA or Twilio. Through a web application interface, a clinician could setup questionnaires and track a patient's response history in order to enhance the spectrum of care. One can imagine a tie-in with IRIS in order to share and coordinate this patient information with other relevant clinical applications.
Figure 3: Clinical Questionnaire Engine Prototype Design

Testing the Concept
As a follow-up experiment in early 2010, the questionnaire-based interactive voice response application prototype concept was built and tested as an academic exercise within an IRAP-funded project to help entrepreneurs explore the value of CEAs and the Coral CEA sandbox. The result of this initiative was a demonstration web portal that tied together Coral CEA call-conference management web services and an isolated asterisk system which was able to interact with a locally-registered X-Lite SIP softphone in order to setup, place, and record simulated medication-compliance questionnaire calls. The system used pre-recorded text-to-speech voicefiles (to simulate a dynamic engine) linked with questions, together with clinician-supplied call-flow logic, that formed a typical call-out patient compliance questionnaire.
Using database-registered input and action codes associated with questionnaire voicefiles, the system was able to determine the sequence of questions to play for the patient during a call, based on key-digit responses received. The Coral CEA sandbox services provided the ability to create a simulated emergency conference call between a patient and emergency attendant staff using a secondary tie-in application that monitored call state and question responses. In the event of an emergency condition, the patient was asked to hang-up the phone and to expect an immediate call from the nursing staff. The system was then tasked with:
-
Acquiring a call session with the monitoring staff.
-
Providing an automated notification of the situation once a connection was made.
-
Attempting a third-party conference-call with the patient.
Figures 4 through 6 provide a high-level visual representation of the prototype's clinician web interfaces and general functionality. The prototype's logo, licensed under a Creative Commons Attribution 3.0 License.
Figure 4 shows the initial web portal screen following authenticated login by the clinician. The screen to the right is a capture of the patient setup tab, within the web portal's clinician management area. In this space, the clinician can register patients within the application, and find or modify existing patient profiles.
Figure 4: Demonstration Prototype Post-Login and Patient Setup Views

Figure 5 depicts the clinician's questionnaire setup section of the prototype's web portal. Here, the clinician can sample pre-loaded questions in the application's database, organized by category and function type (e.g. generic or relevant to a particular condition or medication). Questions can be added to a questionnaire editing area, where question ordering and response logic can be modified.
Figure 5: Questionnaire Setup Functions

Once questionnaires have been added to the system, the clinician is able to view general logic and call flow via a separate dashboard area. In Figure 6, a sequence of callout questionnaire events is shown:
-
A clinician schedules a questionnaire call event for a given patient.
-
The system confirms the scheduling request.
-
According to the start time, frequency, and duration parameters provided, the call manager organizes call queue events within the asterisk system. A tested call is shown in the last frame as tested using a registered X-Lite SIP softphone client.
Figure 6: Test Call Setup and Execution

Conclusion
The application of collaborative frameworks in the healthcare domain provides an opportunity for innovation and leadership in an arena traditionally dominated by large-scale IT initiatives. Increasing pressure by federal and provincial governments to implement a common EHR system across Canada and mature open source driven telecommunications stacks have provided the foundation for a collaborative revolution in healthcare delivery. Entrepreneurs seeking to innovate in this space should heed the message of collaboration and partnership, leveraging commoditized data-management services from provincial EHR infostructures. Similarly, innovations in community-led CEA infrastructure development should play a pivotal role in expanding shared provincial communications infrastructure capacity and standards to support periphery application innovation.
Recommended Resources